Authorization For Use And Disclosure Of Protected Health Information Form
Msdh form 99 page 1 of 2 revised 7202018 authorization for the usedisclosure of protected health information form 99 purpose to provide a means for msdh patients or employees to authorize the release of their health. By completing this form you are authorizing your plan to use or disclose your protected health information as defined by law for the purpose stated below.
authorization for use and disclosure of protected health information form
authorization for use and disclosure of protected health information form is important information with HD images sourced from all websites in the world. Download this image for free by clicking "download button" below. If want a higher resolution you can find it on Google Images.
Note: Copyright of all images in authorization for use and disclosure of protected health information form content depends on the source site. We hope you do not use it for commercial purposes.
Part i section a.

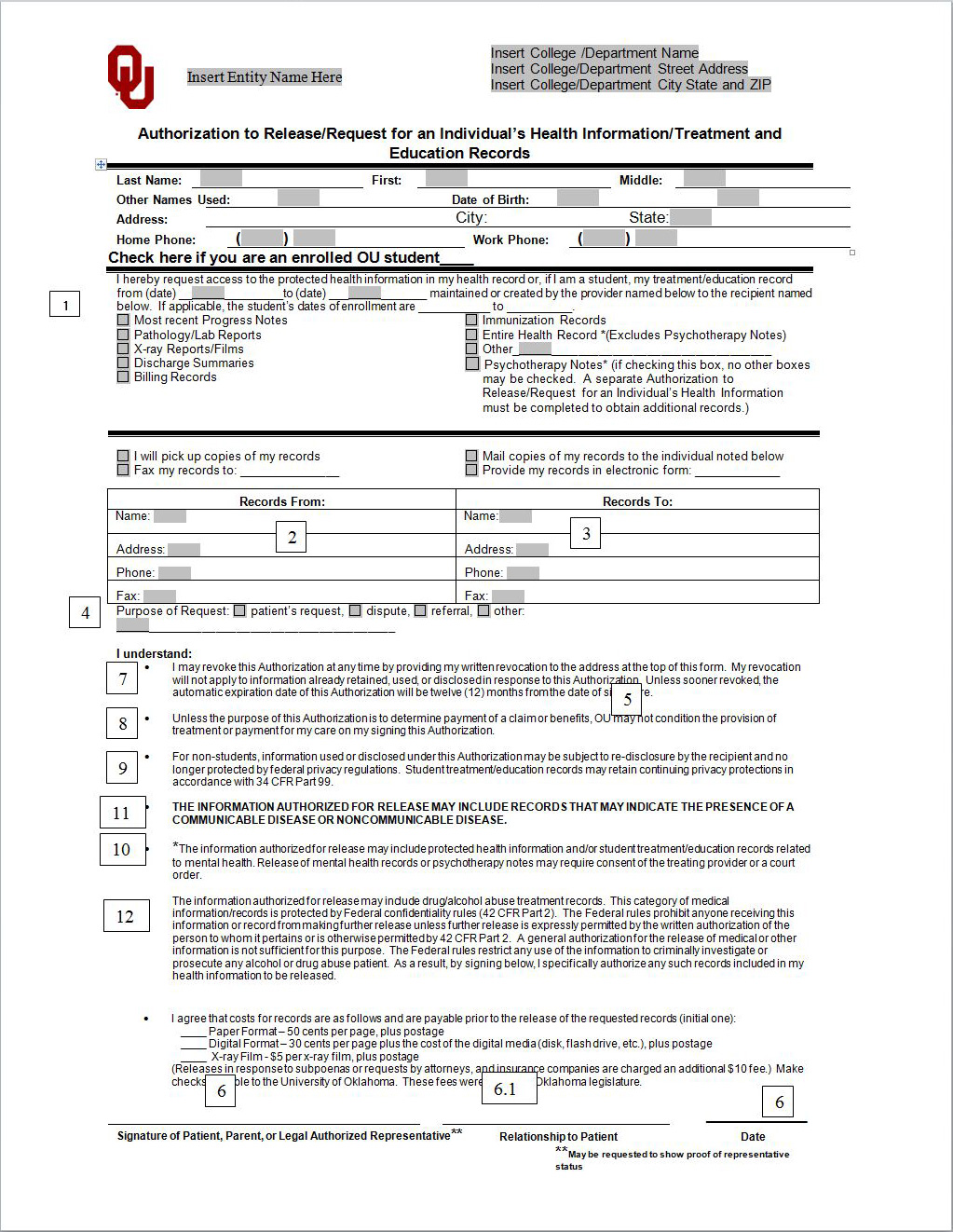
Authorization for use and disclosure of protected health information form. Part ii of this form lets you name someone else to act on your behalf. Authorization is required for the use or disclosure of psychotherapy notes or research health information. 02 29 2020 see omb statement on reverse.
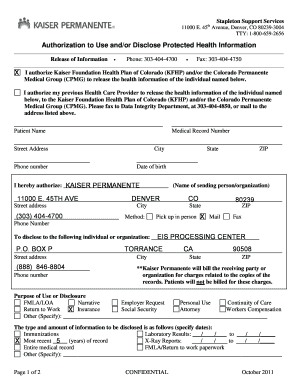
Authorization for use disclosure of protected health information form part i of this form lets la. Hipaa authorization for use or disclosure of health information this form is for use when such authorization is required and complies with the health insurance portability and accountability act of 1996. Please fill out this form and send it to the address above.
Care use or share your protected health information phi with others. Department of health and human services. Omissions in connection with the access use or disclosure of health information obtained through use of the form.
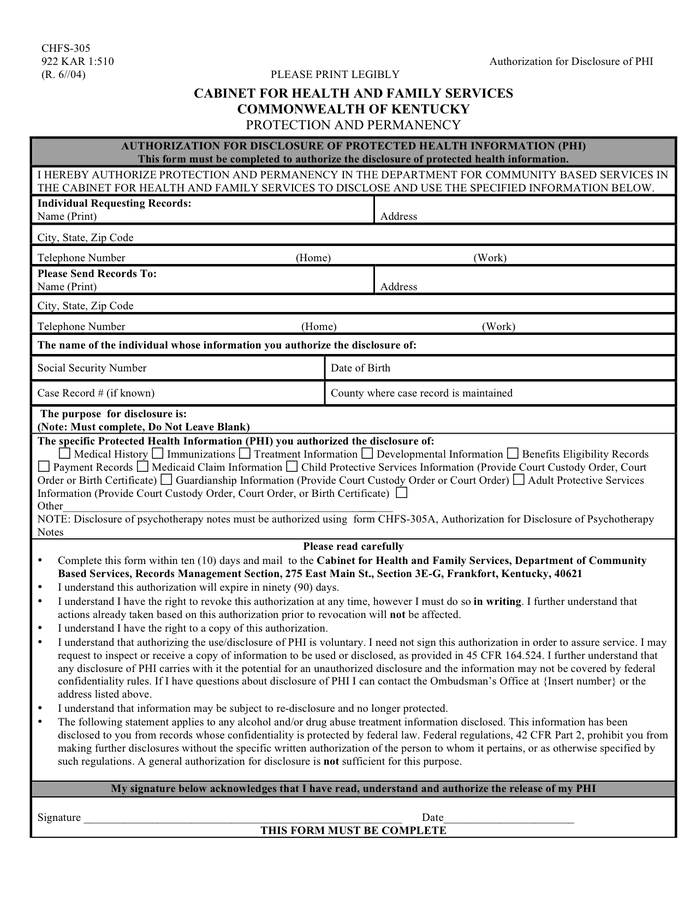
A different authorization form needs to be completed for hospital record 916 854 2000 radiology imaging 916 733 3301 and billing record 916 379 2804. I name of patient hereby voluntarily authorize the disclosure of. The attorney general of texas has adopted a standard authorization to disclose protected health information in accordance with texas health safety code 181154d.
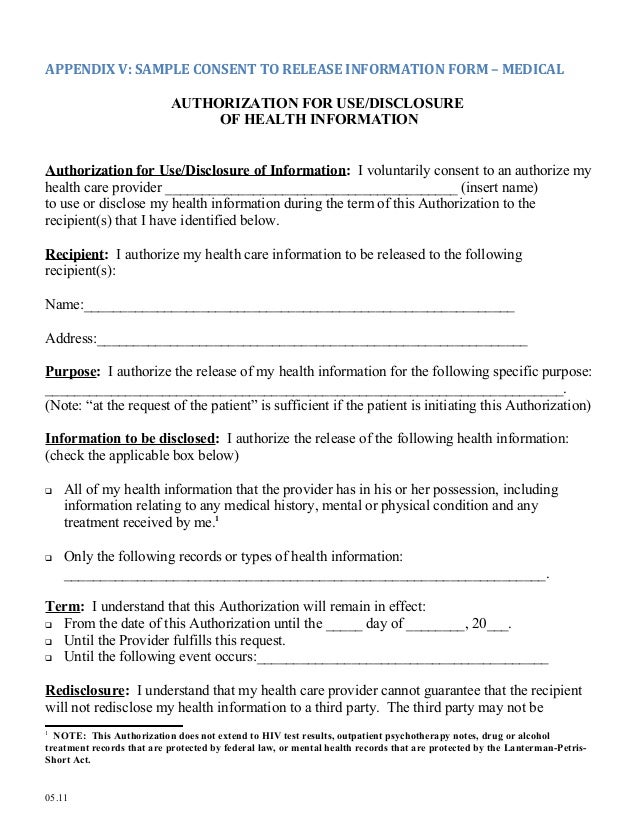
Use of this form does not exempt any entity from compliance with applicable federal or state laws or regulations regarding access use or disclosure of health information or other sensitive personal information eg 42 cfr part 2 restricting the use of information pertaining to drug alcohol abuse and treatment and does not entitle an. Authorization to health advocate to use and disclose your protected health information. Last two years clinic records will be released.
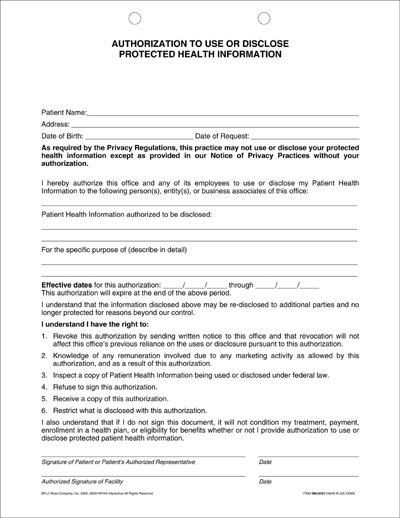
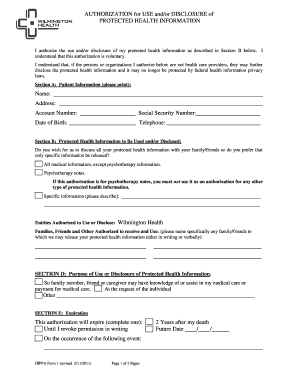
We may disclose protected health information with contracted service providers. If you would like to authorize release of psychotherapy notes you must complete the authorization to use or disclose. Authorization for use or disclosure of protected health information when you complete and sign this form health information about you will be released as you describe in the form.
Please read each section carefully and complete the required sections before signing. Authorization for use or disclosure of protected health information. Complete all sections date and sign.
We may disclose protected health information. Disclosure we will use and disclose protected health information as necessary to administer health advocates programs. Hipaa authorization for use or disclosure of health information.
This form may not be used to authorize release of psychotherapy notes.
 Delaware Authorization For Use Or Disclosure Of Protected Health
Delaware Authorization For Use Or Disclosure Of Protected Health
Https Pottstown Towerhealth Org App Files Public 21 Auth To Releasemed Info Form Pdf
 Bill Of Sale Form California Authorization For Use Or Disclosure
Bill Of Sale Form California Authorization For Use Or Disclosure
 Authorization To Use And Disclose Individually
Authorization To Use And Disclose Individually
 Medical Release Form
Medical Release Form
 Bill Of Sale Form Delaware Authorization For Use Or Disclosure Of
Bill Of Sale Form Delaware Authorization For Use Or Disclosure Of
 Hipaa Compliant Authorization Form For Use Or Disclosure Of
Hipaa Compliant Authorization Form For Use Or Disclosure Of
 Hipaa Frequently Asked Questions Faqs The University Of
Hipaa Frequently Asked Questions Faqs The University Of
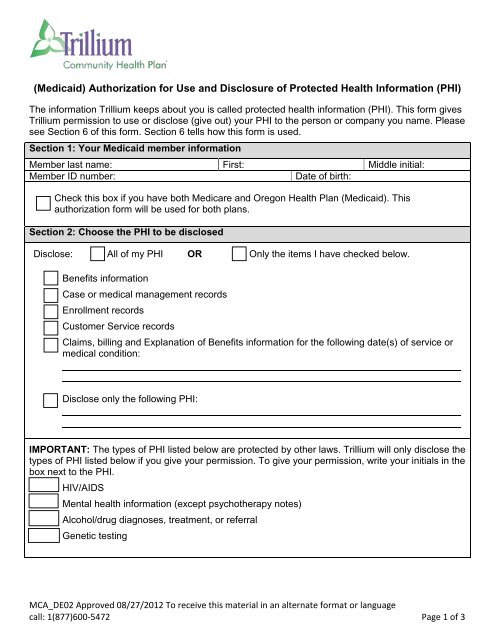 Authorization Disclose Personal Health Information Trillium
Authorization Disclose Personal Health Information Trillium






0 Response to "Authorization For Use And Disclosure Of Protected Health Information Form"
Post a Comment